I spent most of my life being told what I had was rare, complex, or not well understood. None of those framings produced a treatment plan. This is the one that did.
For my entire life I have lived with hypermobile Ehlers-Danlos syndrome (hEDS) and mast cell activation syndrome (MCAS) — conditions that produced chronic pain, severe joint instability, and multisystem symptoms that took decades to name correctly. Diagnostic delays, multiple spinal fusions, and joint repairs were the early chapters. The later chapters look different: regenerative medicine, orthobiologics, exosome therapy, and structured rehabilitation that respected my surgical history. The combination is what rebuilt function.
This is the case study that sits underneath everything else I write here. It covers:
- The interaction between connective tissue fragility in hEDS and mast cell-driven inflammation
- How exosome therapy and PRP stabilized tissue around prior surgeries
- The systemic effect of 15 years of Botox — and what happened when I stopped
- How stellate ganglion blocks and neuro-reset protocols changed dysautonomia
- A long-arc strength-building protocol built around implants, not against them
The three conditions, and why they amplify each other
Hypermobile Ehlers-Danlos syndrome (hEDS). A genetic connective tissue disorder producing joint hypermobility, skin fragility, and chronic pain. I mapped my own genetics and found a stack of individually “benign” variants in collagen genes (COL5A2, COL4A4, COL17A1) and in methylation pathways. Stacked, they are not benign. hEDS frequently overlaps with dysautonomia, including POTS.
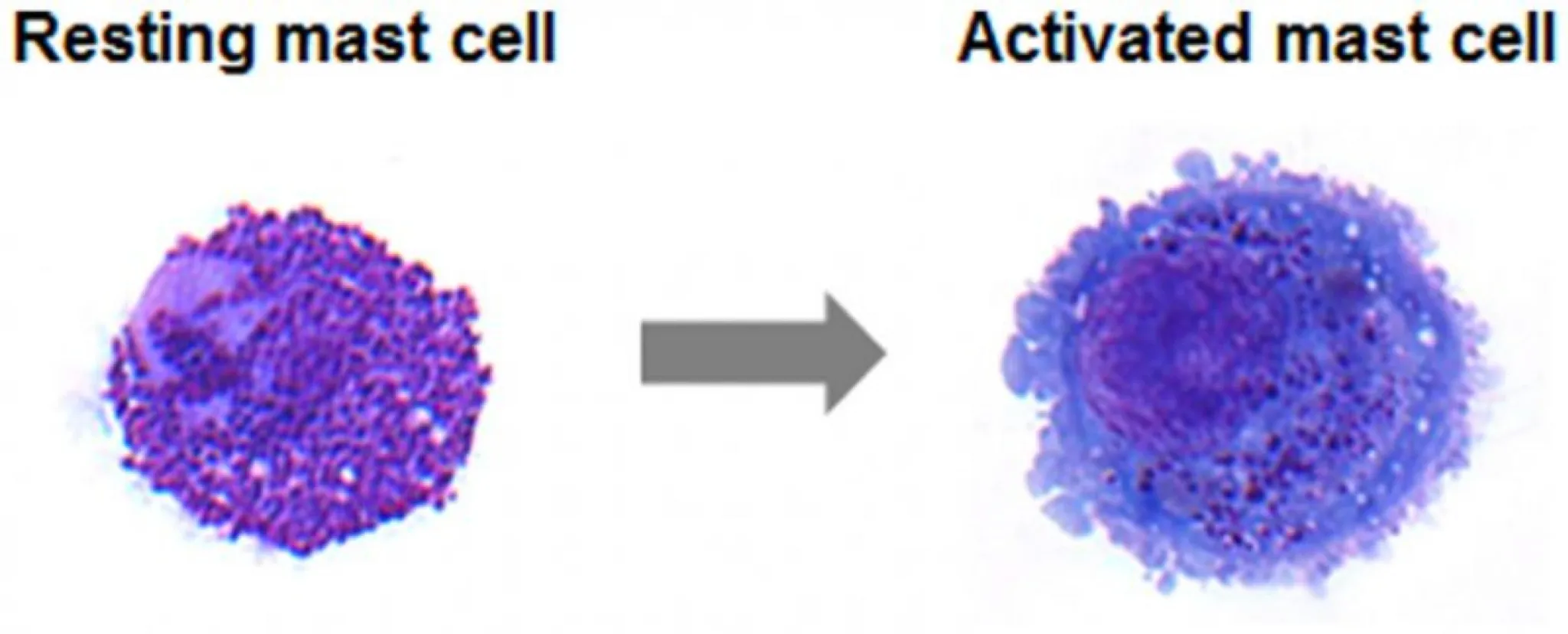
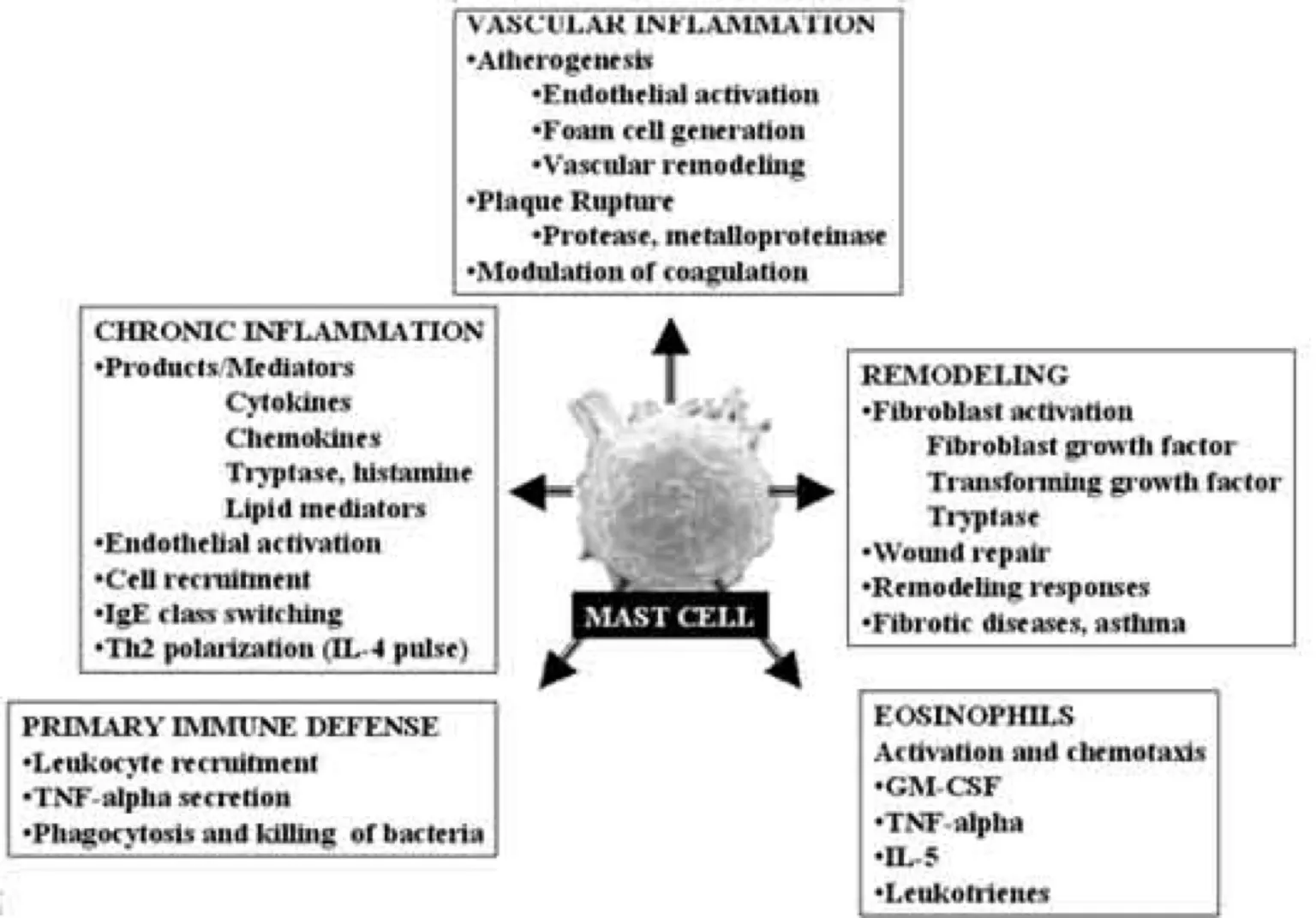
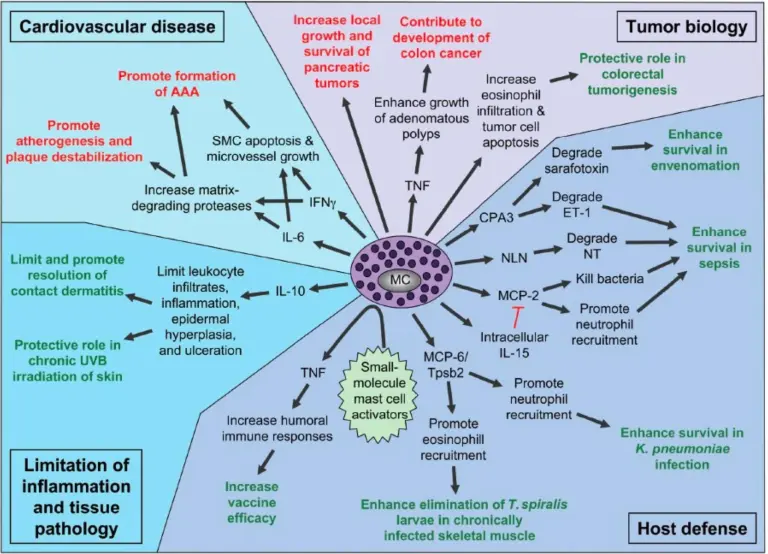
Mast cell activation syndrome (MCAS). Overactive mast cells release histamine, tryptase, and MMP9. The histamine drives vasodilation and increased venous compliance — worsening dysautonomia. The MMP9 actively degrades collagen — worsening joint instability. The two conditions don’t just coexist; they accelerate each other.
Fibromyalgia and central sensitization. The nervous system amplifies pain signaling on top of an already inflamed system, creating a self-perpetuating loop that earns the term inflammaging.
The composite picture: genetically weak collagen, mast cell-driven inflammation that degrades collagen further, and a nervous system that wires the whole thing into chronic alarm.
In hEDS, the body is bendy, but the spirit must not break.
The clinical arc
Childhood through young adulthood. Back pain at 12. A high school diving accident produced a spinal concussion and disc rupture. In medical school I was misdiagnosed with anxiety. Dysautonomia symptoms — POTS, temperature dysregulation, tachycardia, arrhythmia — became unignorable in my twenties.
Trauma and surgeries.
- A severe bus accident fractured both pubic rami and my sacroiliac joint, requiring surgical fixation.
- 2016-2017: three-level cervical artificial disc replacement (ADR) with Professor Dr. Bertagnoli in Germany, after progressive neurological decline with loss of sensation and reflexes forced urgent surgical management. Had this been caught earlier, regenerative medicine might have been sufficient.
- Three-level cervical fusion plus regenerative spine work for atlantoaxial instability with Dr. Fraser Henderson and Dr. Marko Bodor.
- Complications across these surgeries included post-surgical anaphylaxis, arrhythmias, and severe wound-healing failures — internal muscle stitches ripped, leaving a four-inch dehiscence.
The combination that pulled me out — orthobiologics, PRP/PRF/PRGF, exosomes, neuro-regulation, and targeted rehab — was assembled by trial and error over a decade.
Healing is not about erasing pain, but about understanding its language and learning to move with it, not against it.
What regenerative medicine actually did
Orthobiologics and exosomes. Hundreds of PRP and exosome injections across the lifespan of my injuries, plus hyperbaric oxygen — for which I had to petition my insurer when I had a non-healing surgical wound. Regenerative peptides (BPC-157, TB-500, thymosin alpha) for inflammation modulation.
Stellate ganglion blocks and neuro-reset. Six cycles of bilateral stellate ganglion blocks (SGB) substantially improved dysautonomia and autonomic regulation, and helped move me toward remission. Neuro-reset protocols with Dr. Kuo at Extension Health and Dr. Cook at Bioreset added vagal and pharmacologic layers I had not been able to access from a stellate block alone.
Botox — and what happened when I stopped. I had ~20 units of Botox every 4-6 months for fifteen years, for tension headaches and aesthetics. When I discontinued, I saw measurable strength gains. Botulinum toxin can produce systemic muscle effects beyond the local injection site — the case literature documents this at high cumulative doses, but the mechanism is worth weighing if you have a connective tissue disorder where muscle is doing the work that lax ligaments cannot.
Regenerative therapy was central to tissue stabilization and inflammation control. It was not magic. It was a tool that worked because it was sequenced correctly with the rest of the protocol.
The biology underneath
Genetic variants. COL5A2, COL4A4, COL17A1 → collagen dysfunction. MTHFR and glutathione synthase variants → impaired detoxification and elevated systemic inflammation. The supplementation plan I run now (Thorne Methylgard Plus, SAM-e, lysine, pregnenolone with boron) was assembled around these specific deficiencies.
MCAS and MMP9. Mast cell degranulation releases histamine, which produces vascular fragility. MMP9 upregulation actively degrades the collagen substrate of my joints. Tracking MMP9 during flares gives me an objective handle on what is otherwise a felt experience.
Strength training around implants.
- Progressive loading without axial compression to protect the artificial discs.
- Eccentric and isometric loading for tendon and ligament work. Never push through clicking, snapping, or pain.
- Functional rehabilitation aimed at restoring movement patterns rather than chasing peak loads.
What ten years of trial and error taught me
Personalized care matters. Generalist specialists did not help me. Specialists in orthobiologics, regenerative medicine, and functional health did.
Self-advocacy needs data. Documenting genetic results, biomarkers, and treatment responses is the difference between treatment plans that converge and treatment plans that drift.
Surgery is step one, not the answer. Post-surgical rehab, neuro-reset, and progressive strength-building did more for my long-term function than the surgeries themselves. Both were necessary.
What this case study is for
For patients: the message is that the order matters. Diagnose first. Stabilize the spine before the extremities. Control mast cells before chasing tissue repair. Reset the nervous system so the regenerative work has somewhere to land.
For clinicians: the message is that the overlap between hEDS, MCAS, and dysautonomia is mechanistic, not coincidental. MMP9 is a tractable biomarker. SHBG and free testosterone tell you something about whether the system is recovering. Botox in chronic users may not be benign. And patients who have done their genetic homework are not making things up.
This is one person’s data. It is also a working protocol assembled from primary literature and a decade of careful iteration.
A body built on fragile scaffolding demands precision, not force. Strength is earned through patience.
Not medical, legal, or regulatory advice. As of May 2026: no exosome product has FDA approval for therapeutic use; several cell therapies are FDA-approved (HSCT, CAR-T, sickle-cell gene editing, Ryoncil for graft-versus-host disease) but none for the orthopedic or regenerative-medicine indications discussed here. A few states — Texas, Florida (effective July 2025), Utah, Mississippi — have created limited permission frameworks for certain non-FDA-approved stem cell therapies; none extend to exosomes, and federal law still preempts. Full regulatory rundown →